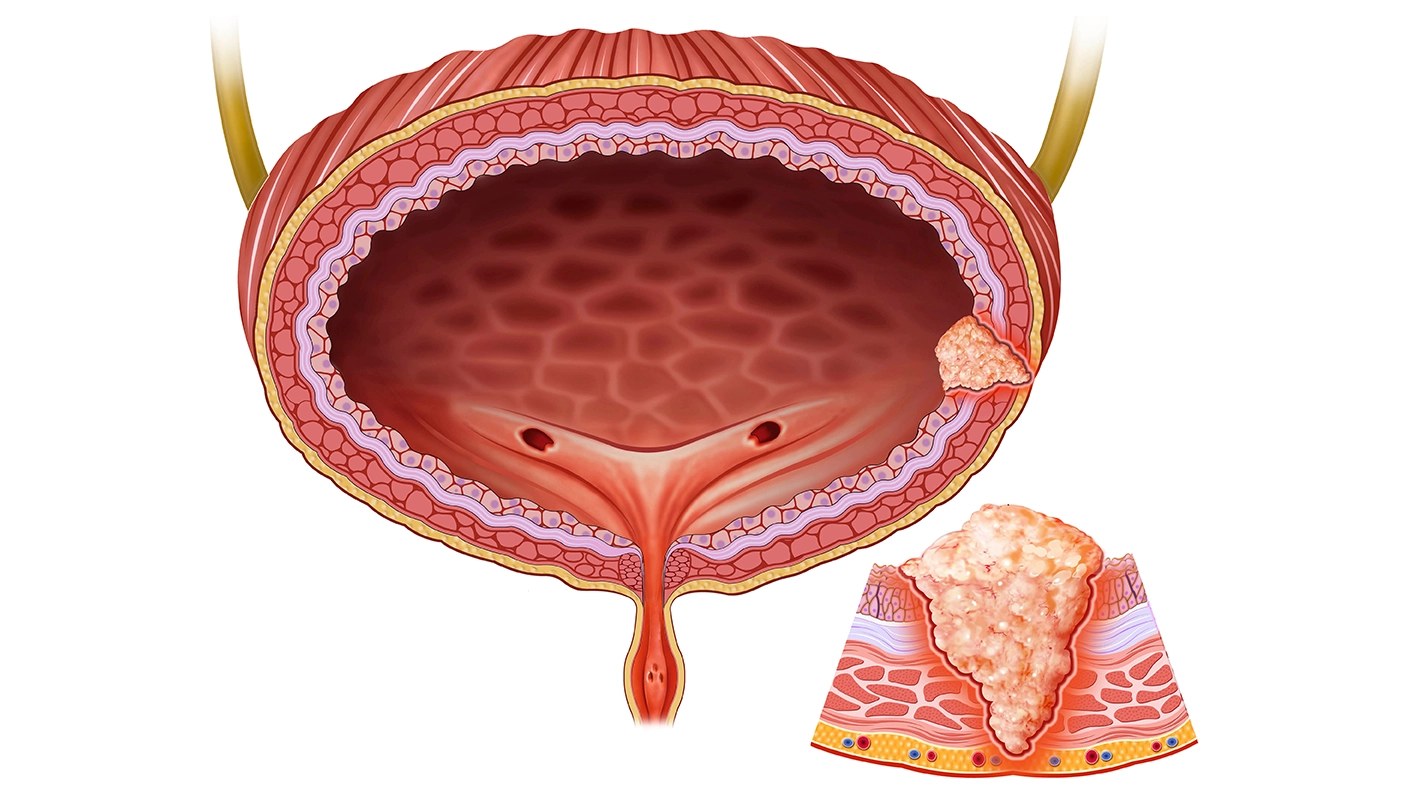
AUA 2026: Updates on Management of Non-Muscle Invasive Bladder Cancer






Dynamic Prediction of Recurrence and Progression Risk in Non-Muscle Invasive Bladder Cancer Using Conditional Survival: A SEER-Medicare Analysis
Authors: Chia-Xhen Chang, Agustin Perez-Londoño, Jamil Almohtasib, Sumedh Kaul, Aaron Fleishman, Simon Kim, Aria F. Olumi, Peter Chang, Andrew Wagner, and Boris Gershman
This SEER-Medicare study evaluated conditional recurrence-free survival (RFS) and progression-free survival (PFS) in older adults with non-muscle invasive bladder cancer (NMIBC). The analysis included 39,862 patients aged 66–89 years with Ta, T1, or carcinoma in situ (Tis) bladder cancer treated with transurethral resection of bladder tumor (TURBT). Median follow-up was 65 months. At baseline, 60-month RFS and PFS rates were 0.39 and 0.85, respectively. Conditional 60-month RFS improved progressively with longer event-free intervals, increasing from 0.52 at 6 months to 0.85 at 60 months. Conditional 60-month PFS also improved from 0.86 at 6 months to 0.91 at 60 months. Improvement in recurrence-free survival was most pronounced during the first 24 months and was greatest in patients with T1 disease. Over time, tumor stage and grade became less predictive of recurrence-free survival. Overall, recurrence and progression risks decreased with longer event-free survival, supporting the use of dynamic risk prediction during follow-up of NMIBC.
Prognostic Outcomes Comparing Upfront Radical Cystectomy and Primary BCG Therapy in Very-High Risk Non-Muscle Invasive Bladder Cancer: An Updated Analysis in the Modern BCG Era
Authors: Sagar Patel, Zhouxuan Li, Joseph Black, Wei Qiao, Mikael Rauf, Taeweon Lee, Kelly Bree, Charles Guo, Byron Lee, Colin Dinney, Neema Navai, and Ashish Kamat
This retrospective study compared outcomes of primary Bacillus Calmette-Guérin (BCG) therapy versus upfront radical cystectomy (RC) in patients with European Association of Urology (EAU)-defined very-high risk (VHR) non–muscle invasive bladder cancer (NMIBC). Among 285 patients with VHR NMIBC, 166 received primary BCG therapy and 119 underwent upfront RC. Median follow-up was 51 months. Variant histology was more common in the RC group (43% vs 17%; p<0.001), while rates of T1 disease, carcinoma in situ (CIS), lympho-vascular invasion (LVI), and prostatic urethral involvement were similar between groups. At 5 years, overall survival (OS) was 82% in the BCG group and 76% in the RC group (p=0.71). Cancer-specific survival (CSS) was 96% versus 95% (p=0.67), and progression-free survival (PFS) was 71% versus 70% (p=0.59) for BCG and RC, respectively. Survival and progression outcomes were comparable across all EAU-defined VHR subgroups, regardless of the number or type of risk factors. Overall, primary BCG therapy demonstrated outcomes comparable to upfront radical cystectomy in patients with VHR NMIBC.
Predicting Cancer-Specific Mortality in Non-Muscle-Invasive Bladder Cancer: Comparative Performance of AUA vs EAU Risk Classifications
Authors: Mattia Longoni, Pietro Scilipoti, Mario de Angelis, Paolo Zaurito, Giovanni Tremolada, Alfonso Santangelo, Giuseppe Simone, Riccardo Mastroianni, Chiara Lonati, Stefania Zamboni, Nazareno Suardi, Gautier Marcq, Aleksandra Szostek, Jorge Caño Velasco, Alfonso Lafuente Puentedura, José Daniel Subiela, Pedro del Olmo Durán, Aleksander Ślusarczyk, Pierre I. Karakiewicz, Benjamin Pradere, Francesco Soria, Paolo Gontero, Morgan Roupret, Francesco Montorsi, Andrea Salonia, Alberto Briganti, and Marco Moschini
This multicentre European study evaluated the ability of the European Association of Urology (EAU) and American Urological Association (AUA) risk classifications to predict cancer-specific mortality (CSM) in patients with non-muscle-invasive bladder cancer (NMIBC). The analysis included 2,192 patients treated with transurethral resection of bladder tumor (TURBT) between 2015 and 2022. According to EAU criteria, 23% were classified as low-risk (LR), 45% as intermediate-risk (IR), 27% as high-risk (HR), and 5.6% as very high-risk (VHR). Median follow-up was 49 months. Using the EAU classification, 2- and 5-year CSM rates were 0.0% and 1.3% for LR, 2.3% and 4.5% for IR, 7.1% and 14% for HR, and 6% and 15% for VHR patients, respectively. The EAU model showed better predictive accuracy for CSM than the AUA classification, with higher area under the curve (AUC) values at both 2 years (0.70 vs 0.58; p=0.028) and 5 years (0.75 vs 0.61; p=0.001). Overall, the EAU classification demonstrated superior prognostic performance for predicting cancer-specific mortality in NMIBC.
BCG Therapy Reshapes the Urinary Microbiome and Immune Cell Landscape in Non–Muscle-Invasive Bladder Cancer
Authors: Yuki Oda, Makito Miyake, Kazuki Miyazaki, Nobutaka Nishimura, Akira Tachibana, Mitsuru Tomizawa, Takuto Shimizu, Kenta Onishi, Shunta Hori, Yosuke Morizawa, Daisuke Gotho, Yasushi Nakai, Tatsuo Yoneda, Nobumichi Tanaka, and Kiyohide Fujimoto
This prospective single-center study evaluated changes in urinary immune markers and microbiota in 23 patients with non-muscle invasive bladder cancer (NMIBC) receiving intravesical Bacillus Calmette-Guérin (BCG) therapy. Urine samples were collected before transurethral resection of bladder tumor (TURBT), before BCG induction, after BCG induction, and 3 months later. Immune-related transcripts and urinary microbiota profiles were analyzed. Programmed death-ligand 1 (PD-L1) and programmed death-ligand 2 (PD-L2) expression increased significantly after BCG induction (p=0.003). CD33 and macrophage scavenger receptor 1 (MSR1/CD204) also showed increasing trends. Microbiota diversity did not significantly change over time. Lower levels of Actinobacteria and abundance of Enterobacteriaceae were associated with altered immune marker expression. The Firmicutes/Bacteroidetes ratio and Enterobacteriaceae abundance correlated with PD-L1 changes. Post-BCG immune and microbiota profiles were significantly associated with longer progression-free survival. Overall, BCG treatment was associated with coordinated changes in urinary immune markers and microbiota, suggesting potential utility of urine-based immune–microbiota profiling in predicting treatment response.
Survival Outcomes of BCG only, BCG plus EMDA-MMC, or Upfront Radical Cystectomy in High-Risk Non-Muscle Invasive Bladder Cancers (NMIBCs): A Multicentre Collaborative Study from Two Independent Tertiary Referral Institutions
Authors: Dalila Carino, Francesco Del Giudice, Valerio Santarelli, Amir Khan, Mohammed Gad, Rajesh Nair, Elsie Mensah, Felice Crocetto, Ettore De Berardinis, Youssef Ibrahim, Benjamin Challacombe, Jan Laszkiewicz, Bernardo Rocco, Giuseppe Basile, Ramesh Thurairaja, Timothy O’brien, Muhammad Shamim Khan, Yasmin Abu-Ghanem, Eila C. Skinner, and Benjamin I. Chung
This retrospective study compared outcomes of different treatment strategies in patients with high- and very high-risk non-muscle invasive bladder cancer (NMIBC). A total of 1,178 patients treated between 2009 and 2024 were included. Patients received either Bacillus Calmette–Guérin (BCG) alone (n=852), sequential BCG plus electromotive mitomycin C (EMDA-MMC) (n=249), or upfront radical cystectomy (RC) (n=77). Kaplan–Meier analysis showed no significant differences in recurrence-free survival (RFS) or progression-free survival (PFS) between the BCG alone and BCG/EMDA-MMC groups. Overall survival (OS) was also similar across all three treatment approaches. On multivariable analysis, treatment modality was not independently associated with RFS, PFS, or OS. Survival outcomes were mainly influenced by age, tumor stage, presence of concomitant carcinoma in situ (CIS), and repeat transurethral resection of bladder tumor (Re-TURBT). Overall, the study suggests that patient and tumor characteristics may have a greater impact on outcomes than the specific treatment strategy used in high-risk NMIBC.
Reduced Versus Full Dose BCG Maintenance in NMIBC Patients Treated with Full Dose Induction: A Matched Analysis
Authors: Michael A. O'Donnell, Yair Lotan, Katherine Lajkosz, Jethro C. C. Kwong, Sarah Attia, Willian Ito, Ian M. Mcelree, Avesh Chadee, Girish S. Kulkarni, and Alexandre R. Zlotta
This multicentre retrospective cohort study evaluated outcomes with reduced-dose versus full-dose Bacillus Calmette-Guérin (BCG) maintenance therapy in patients with intermediate- and high-risk non-muscle invasive bladder cancer (NMIBC). Among 989 patients, 625 received full-dose BCG for both induction and maintenance, while 364 received full-dose induction followed by reduced-dose maintenance. After propensity score matching, 606 patients were analyzed, with 303 patients in each group. Median follow-up was 5.9 years in the full-dose group and 5.6 years in the reduced-dose group. The estimated 5-year progression rates were 14% in the full-dose group and 10% in the reduced-dose group (p=0.144). Multivariable analysis showed no significant difference between groups for progression risk (hazard ratio [HR] 0.69; 95% confidence interval [CI]: 0.44–1.11; p=0.13), cancer-specific survival (CSS), or overall survival (OS). However, recurrence-free survival (RFS) was significantly improved in the reduced-dose group (HR 0.53; 95% CI: 0.43–0.67; p<0.001). Overall, reduced-dose BCG maintenance following full-dose induction showed similar progression and survival outcomes compared with full-dose maintenance.
AUA 2026, May15 – 18, Washington, DC.